
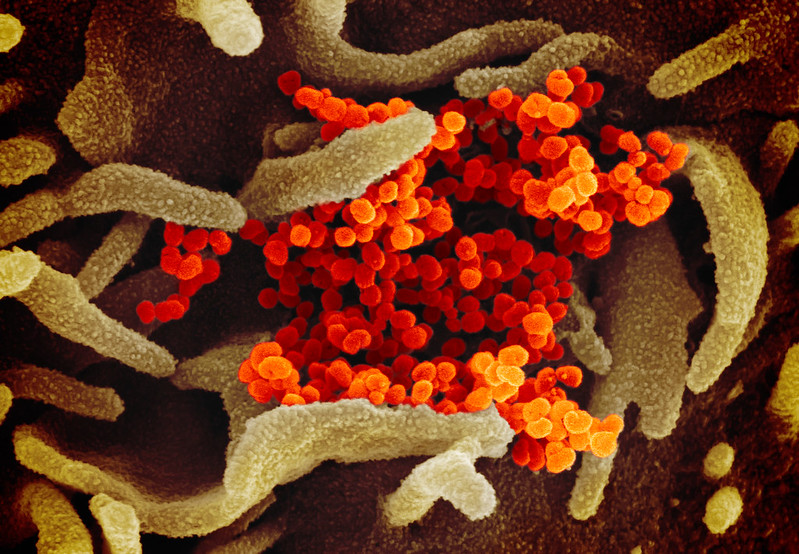
Novel coronavirus, the virus responsible for Coronavirus Disease 2019 (COVID-19) is on the verge of becoming a global pandemic if it isn’t already.
As we stand on the precipice of what could be one of the largest global public health sagas of our lifetimes, I think it’s worth talking about COVID-19 from the “at risk population” perspective. A few days ago the World Health Organization came out and said that those of us living with respiratory illnesses are among the population who could be most affected by the novel coronavirus. While it is definitely not a time to panic, it probably is a time to think about what a “disruption” (as the CDC put it) to normal life could look like.
Just last week I had a quarterly CF visit where I asked a number of COVID-19 questions, namely, should I start stockpiling medicine?
The quarantines around the world certainly have a lot of people on edge, me included to some extent. What is safe? What isn’t safe? Does a mask really protect me?
The relative risk to people in the US is very low, and it’s important we understand that. I do think, however, that preparing for the future is important.
A number of the questions I have are:
Should I start stockpiling medicine?
The answer I received was that I should make sure to strictly follow my refill schedules (a little vague?).
The general population does not rely on chronic medications like we do. Our reliance on the health system exists regardless of what the state of public health looks like. The fear that comes with stockpiling medication creates mounting pressure on the pharmacy network and, in a worst-case scenario, would lead to a run on the pharmacies. That is not what we want (nor do I necessarily think it will happen). That, of course, begs the question, can we even stockpile medicine? The best form of preparation that I can consider at the moment is to make sure we are refilling our scripts as soon as we can. This may not be as big of an issue for people who get 3-month refills, but for those of us who rely on 1-month refills, you are likely feeling the same time sensitive crunch that I am. Most medications and insurance programs allow for 6 weeks of medicine, meaning you can refill your prescription 2 weeks into the 4-week script. That’s the pattern I am following. I recognize my civil responsibility not to contribute to a pharmacy panic, but I know that those of us with underlying conditions require chronic medication and for that reason, as soon as a refill opportunity opens up, I am refilling. Is that stockpiling medication? Maybe. You can be the judge.
Is a surgical mask/respirator the best way to defend against infection?
We’re going to lean on the experts here, and they say, no… probably not (for the general population).
That does not mean we need to abandon respirators in CF clinics and healthcare setting – we are a bit different from the general population.
I am not (for the time being) adding a mask to my everyday routine. Only if I am in a medical setting or flying (which I did 10 days ago, and I was fine), will I wear a mask. Even then, I know it’s not the most effective defense against infection. Personal hygiene – hand washing, not touching your face, avoiding sick people, etc. – will always be the best way to avoid any health issues. I have made an effort to make sure I am thoroughly washing my hands every 30 minutes when I am outside my home. I have no proof to back up my 30-minute hand washing routine, it just gives me some peace of mind.
If you do choose to wear a mask, I can confidently say that the trendy reusable masks – VogMask, Cambridge Mask, etc. – are probably a bad choice right now. Maybe it’s finally time we ditch that trend?
Am I safe at school or work?
It’s unrealistic to think any of us can drop work or school from our daily lives. We depend on paychecks and attendance. Right now there is no reason to believe we aren’t safe at work or school. Where will we draw the line between personal safety and every day life if COVID-19 becomes widespread in the United States, though? The answer to that question may be the same as an answer to another question, what do you do during flu season?
I have to say that I hadn’t necessarily considered the potential severity of COVID-19 until I went to a talk at Dartmouth last week. The keynote presenter was a long time World Health Organization affiliate. After the keynote, Q&A was opened up to the crowd and it felt like I was watching the destruction of civil society as I knew it. While most of the questions were very reasonable scientific inquires, a number of questions from the attendees felt outrageously accusatory. In one case, a Hanover community member (not even a student) comments could have been described as pure panic. She was aware of another community member’s recent return from Italy and was worried about her personal safety through loose affiliation with the traveler’s parents. The keynote speaker, a lawyer by training, was not qualified to answer the question, nor did the question actually relate to anything discussed in his talk. To the surprise of us in the crowd, though, the New Hampshire State Epidemiologist also attended the talk and quickly jumped into the discussion. After a tense back and forth, I felt confident that the public health mechanisms in place will effectively protect us, despite both the official from New Hampshire and the keynote speaker saying that COVID-19 is coming to the United States, if it isn’t already here.
The question I feel most at odds with is: Will we fall victim to healthcare rationing?
My biggest takeaway from the talk at Dartmouth last week was that in the keynote’s perspective, he felt as though the safety of the world was at odds with the safety for the people living in Hubei province where the outbreak started. He then asked, are we willing to sacrifice the civil liberties for the people in Wuhan for the safety of the global community? Further, he wondered if the same would happen here in the US. The example he gave is that there simply are not enough life support machines, isolation units and ICU’s for everyone, despite the enormous steps taken to contain the virus. The irony I felt in the experience of going to the talk was the quasi-panic that ensued in the example I gave above. Really, it all came back to the idea of rationing healthcare, who is protected and why, and “are we safe?” It goes without saying that the context for the discussion concerned a worst-case scenario, one that he said himself didn’t look all that plausible. Rationing is something that largely does not exist in the United States, so it would come as a shock to a lot of us. From my perspective, what does rationing look like for us? If we are the “at risk” population, do we get everything that’s left over or are we the priority? I think this is the question that scares me most.
It’s worth saying that to this point I have not seen anything that specifically relates to the cystic fibrosis community and coronavirus beyond the few candid conversations I had with my doctors, and that includes… what would actually happen to one of us if we contracted the disease? Just as there isn’t any info to suggest we would greatly suffer, there’s just as much of a lack of information to suggest it would or would not be as violent as a flu infection. Further, I think it is worth reiterating that the CDC is the global leader on infectious disease containment, and I have all the faith in the world in the organization.
I would, however, like for the Cystic Fibrosis Foundation to make some sort of comment on the situation. I can sense some unease from our patient population largely because the topic is all over the news. It felt like my CF clinic was waiting for guidance as well. They had discussed the matter internally, but nothing concrete has come down as far as the risk goes for our community as a whole.
It’s perfectly fine to be unsettled, but is it time to panic? Probably not. That doesn’t mean you should not prepare. I did. Some of the steps I have taken so far include:
- Refill all available scripts and write out a schedule to make sure that I have the maximum allowable medication on hand per my insurance. (I will say that we have NOT gotten any indication from our industry partners that there is reason to suspect supply chain disruptions.)
- Maintain stocks of “over the counter” cold and flu medicine (mostly for fevers).
- Buy an extra supply of water and food, enough to last 2-4 weeks in the event of a local outbreak, and thus self-imposed isolation.
- Create a plan with my care providers. Last week at clinic, I brought up COVID-19 and asked what my plan should be should not only there be a local outbreak, but also in the unlikely event that I contract the disease.
- Slowly build a stock of household items like toilet paper, disinfectant wipes, bleach, laundry detergent, etc.
My hope, rather expectation, is that in the coming months we will know a lot more about coronavirus and how our “at risk population” can better prepare, or if we even need to be preparing beyond what we are already doing.
If anything… I’m just exited that people are super anal about washing their hands. I call that a win.



