Just this afternoon, much of the CF Community became aware of a cystic fibrosis and COVID-19 outcome study in Respiratory Medicine. The article was published back in September, but it’s making the rounds on social media today.
This study is of serious interest for our patient community because, at its core, it is really the exact thing we’ve all been waiting for: a comprehensive look at COVID-19 outcomes for people with cystic fibrosis compared with people who do not have cystic fibrosis.
Of course, with stuff like this, emotions run hot, and the big takes are out there on the Internet. But what does it all really mean? Biostatistics and epidemiology are like their own little languages, so sometimes it can be hard to interpret the findings on a microlevel to help you answer the question, “well, what should I do?”
The truth is that if you’re reading this paper today and are suddenly running for the hills because it suggests that people with CF are at an elevated risk for poor outcomes due to COVID-19, I’m going to tell you not to run… and then take a deep breath. Join me on an adventure into the data to better understand the information being conveyed.
So, yes, the bottom line is that the researchers did find an elevated risk for people with cystic fibrosis for all three of the outcomes measured in the absence of a vaccine: inpatient services, critical care, and acute renal injury. Yes, people with cystic fibrosis are high risk for serious outcome for COVID-19, but I’ll argue we all knew that anyway.
How to the researchers got to this answer may confuse some, so I’ll do my best to explain it. Essentially, they took two groups of people. On one end, you have 422 people with cystic fibrosis reported to have had COVID-19 and on the other you have 507,388 people without cystic fibrosis who also had COVID-19. People were included in the cohorts if they had COVID-19 between January 20, 2020 and January 9, 2021, meaning in a time before vaccines were widely available for people. From there, the authors used a statistical method to “match” people with cystic fibrosis to people without cystic fibrosis based on a number of different characteristics so that COVID-19 could reasonably be considered the main difference between the two groups. The method they chose was called “propensity matching.” In the end they had two groups of 413 people each. One group including people with CF, the other group including people without CF. Below you can see the data for yourself (I recreated the data in an Excel sheet using the same math the authors did just so it could appear more clearly on my blog). The top chart is unmatched absolute data, which shows the absolute rate of the outcomes in the entire CF and non-CF groups, while the bottom chart shows the matched cohorts and their corresponding risk ratios (to be explained below). I highlighted the three outcomes there showed statistically significant differences between the two cohorts. It might give you some relief to know that 30-day mortality wasn’t statistically different between people with CF and without CF in these matched groups (though it does seem a little high for people with CF).
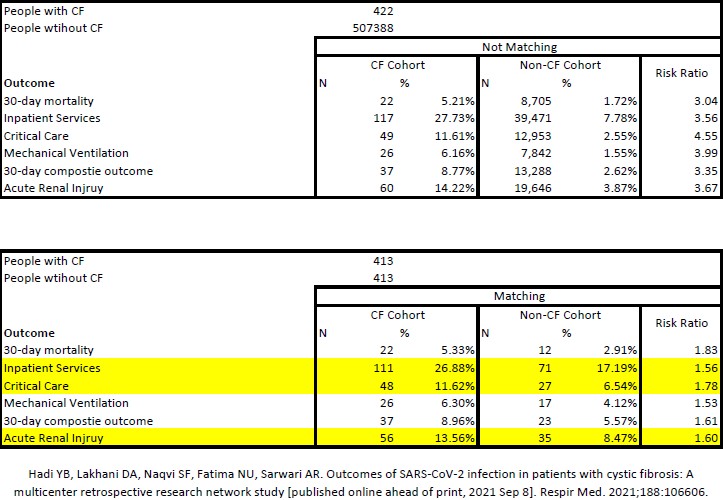
Of the outcomes considered, inpatient services, critical care, and acute renal injury all yielded a statistically significant difference from the matched cohort from a risk ratio perspective.
In plain English, you read a risk ratio as… People with cystic fibrosis are 1.56 times the risk compared to those without cystic fibrosis for inpatient services [hospitalization].
On an absolute level in the matched CF cohort, meaning when I look at just the CF “N” column, I’m stuck by how high the hospitalization rate was (111 of 413 people or ~27%). That’s crazy high, and certainly speaks to the power of vaccination. The same could also be said for critical care (ICU) and acute renal injury, which both commanded risk ratios of 1.78 and 1.60 respectively compared with the non-CF cohort.
Now you might look at the mortality and mechanical ventilation statistics and wonder why I’m not commenting on those specific outcomes. It’s a little bit more complex and dives into some statistical theory, but essentially, I would imagine that the rates just aren’t high enough to draw a conclusion. That doesn’t mean they aren’t meaningful, but the authors didn’t find a statistically significant difference.
With all that said, how does this affect us on an individual level? Only you can answer that. In times like these we are stewards of the data we come across to inform our actions. I take a look at these data and my first thought is… wow, I’m damn glad I got a vaccine. I also feel vindicated for advocating so strongly alongside the rest of the CF community for speedy vaccine access. I’m also pulling my hair out saying… where the hell were these data when we were advocating for vaccines?! We stayed up long nights looking for legitimate hospitalizations rates and couldn’t find any. These data clearly show the risk of hospitalization and inpatient complications are much higher after a SARS-CoV-2 infection for people with CF.
A quick note about the absolute data in the unmatched cohort. The absolute rate of the listed outcomes is important for painting a picture of what is happening to THOSE 422 patients. As another aside, the authors said that modulator therapy appeared to confer some protection, but it wasn’t statistically significant. Now this is where I’m going to sound contradictory. Because the treatment isn’t statistically significant, it doesn’t mean that it’s not clinically meaningful. The answer there is that it… probably doesn’t hurt to be on one.
Further, and importantly, the researchers cited that younger age doesn’t appear to confer protection for people with CF.
If you have already gotten a vaccine, these data may not mean too much to you. It would be wrong to apply these statistics to all facets of life after vaccination. They may be useful to inform further study about outcomes in people with CF who have suffered a breakthrough infection. Because I’m a data nerd, I know I would love to see those data and then COMPARE them to these pre-vaccine data. Talk about a stats analysis!
What do these data not mean? They don’t mean the CF Foundation’s periodic registry data on SARS-CoV-2 infections in CF are wrong. Those data and these data are like comparing apples and oranges. The authors even say: “All of our patients had 30-day follow-up available, during which time their disease course should have truly manifested itself, and therefore this analysis results in a more ‘real world’ and accurate picture of the course of COVID-19 disease in this population.” They use the word “more” to relate their findings to those published stats in registries and other outcome studies. Registry reports (like the ones the CF Foundation sometimes sense out) are important because they can inform absolute rates of disease, but only after follow-up is achieved with another clinical encounter. The authors here have shown that their ability to detect 30-day follow up was crucial to their findings.
Finally, we have to talk about limitations. There was a good chunk of transplant patients included in these data, and because of the immunocompromised state that transplant creates, there could be somewhat of a data skew embedded in here.
Will these data change my life? No, they will not. I’d argue this is something we’ve all known all along. I feel protected behind my vaccines (watching the FDA/CDC over the next couple of weeks for that booster recommendation) and know that I’ve gotten myself this far in the pandemic with my periodic risk tolerance reviews. I’ll keep it up, and so should you!