The cystic fibrosis community can be split into several groups, none more important, though, than our break between adult and pediatric patients.
On one hand we have children, backed by their very passionate parents. On the other side we have adults who have broken through the childhood disease, and are redefining the condition on a daily basis.
Although we are all cystic fibrosis patients and are striving towards the same goal – a livable cure – we have very different needs.
The difference is very simply broken down with a single word – time.
Time is what separates children from adults living with our condition.
Children are granted exponentially more time with each breakthrough, “Our kids born today can live to be X years old.”
Adults don’t necessarily have the luxury to realize the gains to the same level as children because of disease progression.
Median age of death remains around 29.
As we grow older our disease can progress to a state where it becomes critical for us to focus on a way slow progression rather than experiment with things to flip the outcome. It’s a difficult, risky choice for older patients. Generally speaking, children and their parents aren’t faced with that kind of choice.
Simply put, the quality of life for someone who receives a medication that may improve FEV1 by an absolute 9-13% is very different when that starting baseline is around 50% compared to 80% lung function.
Adult patients are faced with the reality of diminished lung function.
Children are receiving disease-altering support in ways that were never possible for us, and as a result we expect disease progression to happen in a very different way for kids.
It’s an amazing thing, really, but while it’s an incredible leap forward, it’s a smaller piece of the puzzle for adults than it is for kids.
Some older patients with significant disease progression have also subjectively reported that newer medications have led to a further decrease in lung function.
Beyond that, we do not have a way to regenerate dead or diseased lung tissue.
Children must always be given every opportunity to succeed in life. That can never change. Our children are the future. They are the embodiment humanity’s hope and direction.
Our adult community cannot be forgotten, though.
Our adult community has gotten us this far. The fundraising for drug development has been on our backs for decades. We have poured countless hours into fundraisers and trials all the while providing critical data points to help bring our community into the golden age of advancement.
Every patient bears that responsibility, but a lot of us have done it for decades.
So when we’re parading around the phrase, “Children born today can expect to live to be X years old!” I can only be left wondering where does that leave adults?
Our adult population, those of us who have made it out of childhood, is running out of treatment options as antibiotics become less and less effective; we are spending more and more time dealing with pulmonary exacerbations; and we see more and more adults heading towards transplant.
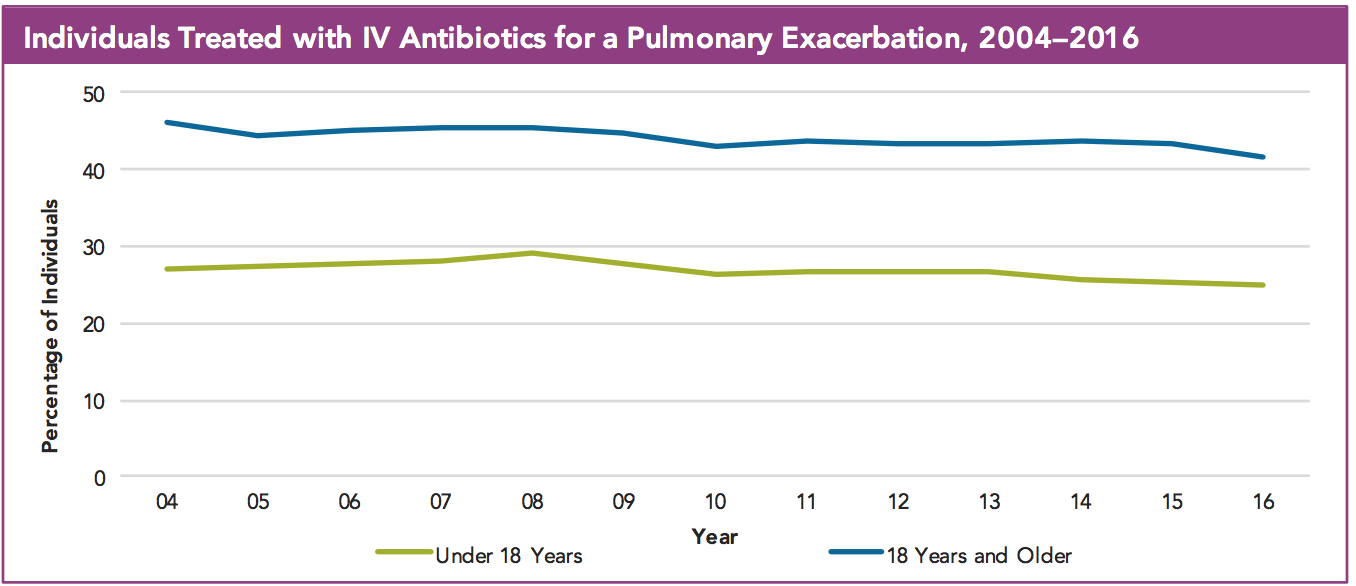
Cystic Fibrosis Foundation Patient Registry Annual Data Report 2016, p. 46 “Pulmonary Exacerbations” – Cystic Fibrosis Foundation
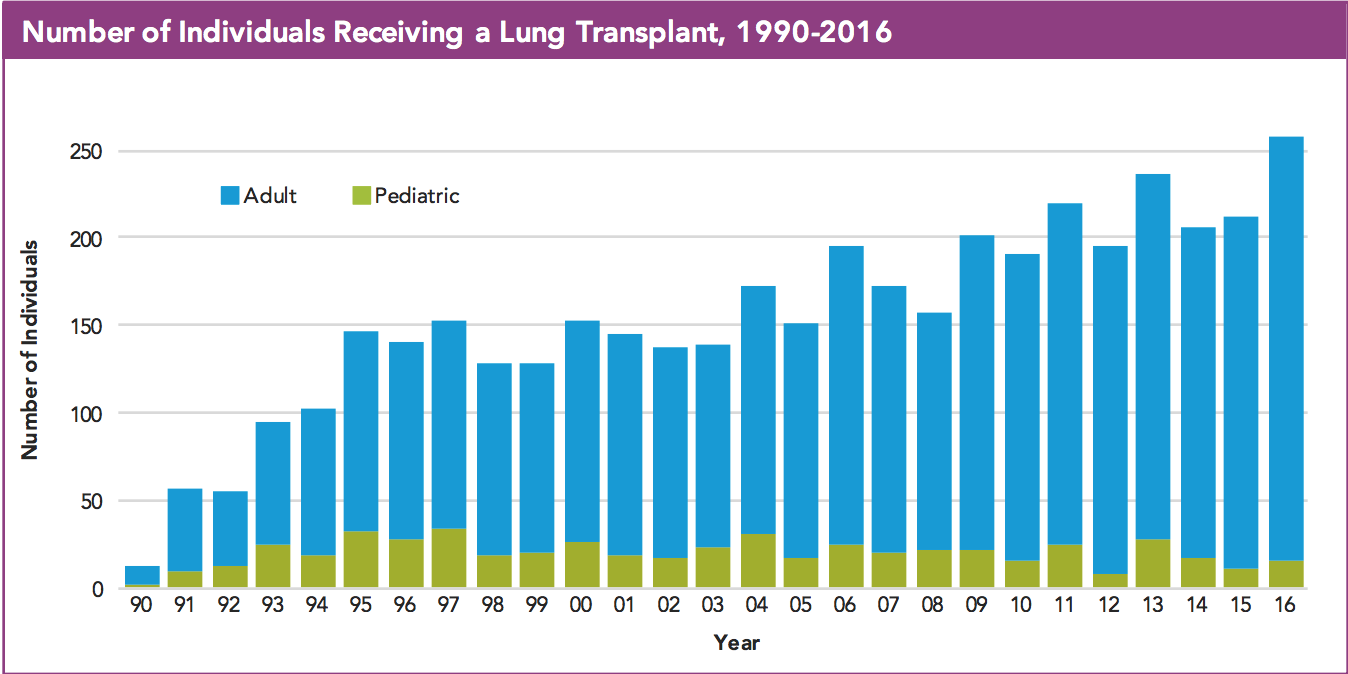
Cystic Fibrosis Foundation Patient Registry Annual Data Report 2016, p. 71 “Lung Transplantation” – Cystic Fibrosis Foundation
Shouldn’t we be working to significantly reduce the need for transplant for the people who have gotten us this far?
Transplant is a scary thought for a lot of people. It’s a dive into the unknown, the utmost risk that people who have been to hell and back shouldn’t have to deal with.
I have never been more excited than now for the future of people living cystic fibrosis, but that doesn’t mean we sit on hands and bask in the glory of achievement.
Right now the best we have is the “Median Conditional Predicted Survival,” which “reflects the population-based median for all individuals of a specific attained age and does not take individual characteristics into consideration.”
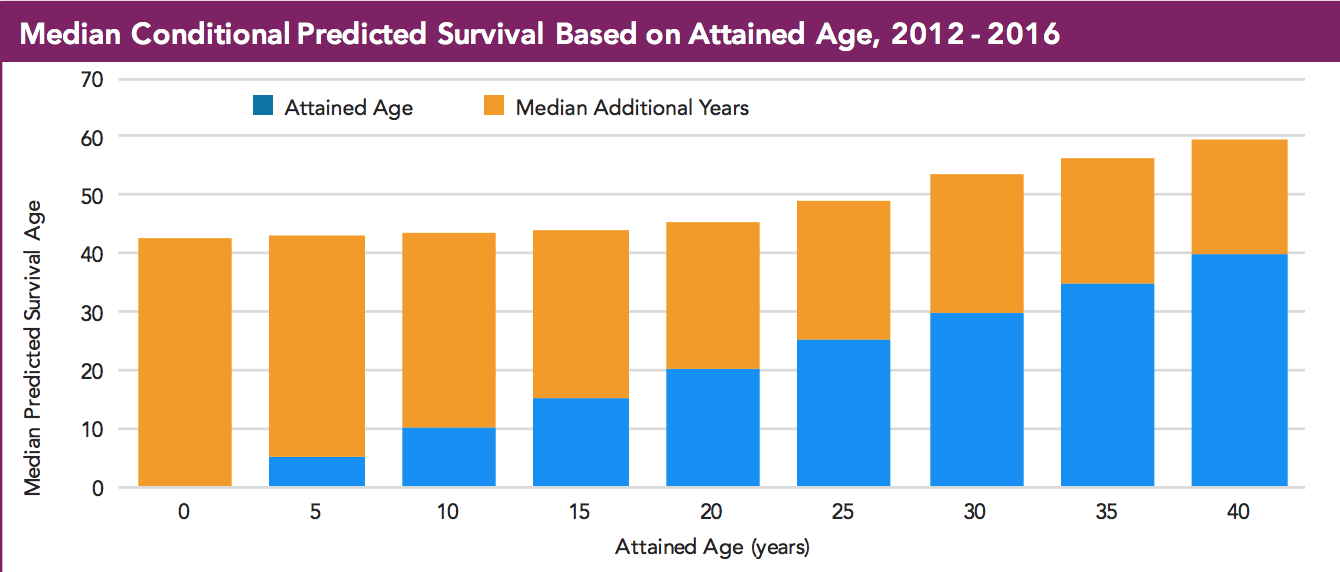
Cystic Fibrosis Foundation Patient Registry Annual Data Report 2016, p. 74 “Survival” – Cystic Fibrosis Foundation
I’m still waiting for the day someone reads a statistic to me that says, “Adults living with cystic fibrosis can expect to achieve a normal human lifespan.”
Main picture credit: Tiffany Rich